Page 40 - Škrgat, Sabina, ed. 2022. Severe Asthma - Basic and Clinical Views. Koper: University of Primorska Press. Severe Asthma Forum, 1
P. 40
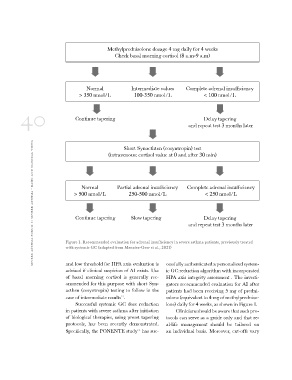
Methylprednisolone dosage 4 mg daily for 4 weeks
Check basal morning cortisol (8 a.m-9 a.m)
Normal Intermediate values Complete adrenal insufficiency
> 350 nmol/L 100-350 nmol/L < 100 nmol/L
40 Continue tapering Delay tapering
and repeat test 3 months later
severe asthma forum 1: severe asthma - basic and clinical views Short Synacthten (cosyntropin) test
(intravenous; cortisol value at 0 and after 30 min)
Normal Partial adrenal insufficiency Complete adrenal insufficiency
> 500 nmol/L
250-500 nmol/L < 250 nmol/L
Continue tapering Slow tapering Delay tapering
and repeat test 3 months later
Figure 1. Recommended evaluation for adrenal insufficiency in severe asthma patients, previously treated
with systemic GC (adapted from Menzies-Gow et al., 2021)
and low threshold for HPA axis evaluation is cessfully authenticated a personalized system-
advised if clinical suspicion of AI exists. Use ic GC reduction algorithm with incorporated
of basal morning cortisol is generally rec- HPA axis integrity assessment . The investi-
ommended for this purpose with short Syn- gators recommended evaluation for AI after
acthen (cosyntropin) testing to follow in the patients had been receiving 5 mg of predni-
case of intermediate results23. solone (equivalent to 4 mg of methylpredniso-
lone) daily for 4 weeks, as shown in Figure 1.
Successful systemic GC dose reduction
in patients with severe asthma after initiation Clinicians should be aware that such pro-
of biological therapies, using preset tapering tocols can serve as a guide only and that re-
protocols, has been recently demonstrated. al-life management should be tailored on
Specifically, the PONENTE study24 has suc- an individual basis. Moreover, cut-offs vary
Check basal morning cortisol (8 a.m-9 a.m)
Normal Intermediate values Complete adrenal insufficiency
> 350 nmol/L 100-350 nmol/L < 100 nmol/L
40 Continue tapering Delay tapering
and repeat test 3 months later
severe asthma forum 1: severe asthma - basic and clinical views Short Synacthten (cosyntropin) test
(intravenous; cortisol value at 0 and after 30 min)
Normal Partial adrenal insufficiency Complete adrenal insufficiency
> 500 nmol/L
250-500 nmol/L < 250 nmol/L
Continue tapering Slow tapering Delay tapering
and repeat test 3 months later
Figure 1. Recommended evaluation for adrenal insufficiency in severe asthma patients, previously treated
with systemic GC (adapted from Menzies-Gow et al., 2021)
and low threshold for HPA axis evaluation is cessfully authenticated a personalized system-
advised if clinical suspicion of AI exists. Use ic GC reduction algorithm with incorporated
of basal morning cortisol is generally rec- HPA axis integrity assessment . The investi-
ommended for this purpose with short Syn- gators recommended evaluation for AI after
acthen (cosyntropin) testing to follow in the patients had been receiving 5 mg of predni-
case of intermediate results23. solone (equivalent to 4 mg of methylpredniso-
lone) daily for 4 weeks, as shown in Figure 1.
Successful systemic GC dose reduction
in patients with severe asthma after initiation Clinicians should be aware that such pro-
of biological therapies, using preset tapering tocols can serve as a guide only and that re-
protocols, has been recently demonstrated. al-life management should be tailored on
Specifically, the PONENTE study24 has suc- an individual basis. Moreover, cut-offs vary